A case of 20year old male with c/o generalized weakness and difficulty in walking since a week
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
CASE PRESENTATION:
A 20year old male pt came with the
1.c/o difficult in walking since 1 week
2.generalised weakness since 1 week
Pt was apparently asymptomatic 3 months back then pt presented with c/o difficulty in walking and generalized weakness for which he went to a local hospital and was diagnosed with hypokalemia and was treated but was not completely resolved. Now pt presented with c/o weakness and difficulty in walking which were aggravated since a week which was insidious in onset and progressive associated with tingling sensation over b/l upper and lower limbs.h/o not able to sense the floor while walking f/b difficulty in holding slippers(cotton wool sensation +).h/o of difficult in getting up from sitting position,difficulty in climbing stairs .h/o not able to button and unbutton his shirt. Pt is able to mix food,comb hair,turn on bed ,get up from lying down position.
H/o nausea and vomiting since a week which was associated with food intake(food particles as contents),non bilious,non projectile,non blood stained.
H/o constipation since a week.
H/o burning micturition since 4 days and decreased water intake since a week.
H/o pedal edema for 2 days which was 7 days back
H/o sob on exertion since 10 days.
NO h/o head trauma,giddiness,convulsions,chest pain,palpitations,cough,cold,haematuria.
PAST HISTORY:
H/o similar complaints of generalized weakness 3 months ago with h/o buckling.He was diagnosed having hypokalemia and was treated in a local hospital.
Not k/c/o DM,HTN,asthma,CKD,CHD,Thyroid anomalies
Non alcoholic and non smoker.No other addictions
HABITS: He was on mixed diet, appetite normal, constipation only on high protein diet
GENERAL EXAMINATION: pt was conscious,coherent,cooperative and well oriented.
No pallor,Icterus,cyanosis,clubbing, lymphadenopathy,edema
Hypopigmented patches were noted over palmar and plantar aspects


VITALS:
Temp: Afebrile on presentation
BP:130/30mmhg on presentation
PULSE:82pm
RR:21cpm
Spo2:98% on RA
CNS :
Higher mental functions intact
SENSORY SYSTEM:intact
Rombergs test:positive (swaying towards right)
MOTOR SYSTEM
Bulk : normal in b/l UL & LL
Tone : normal in b/l UL & LL
Power :
B/l U/L : proximal -5/5 ; distal -5/5
B/l LL:proximal-4/5 ; distal-3/5
Hand grip-100% in both hands
Hand muscles-5/5
Reflexes :
superficial reflexes :
Abdominal reflex: absent
Corneal + ; conjunctival reflex+
CRANIAL NERVES :INTACT
Cerebellar :
Finger nose:+
Finger nose finger:+
Dysdiadokinesia-
Tandem walking-
GAIT:high stepping gait.
PER ABDOMEN:
Soft,non tender
Bowel sounds +
CVS:s1 s2 heard, no murmurs
RS:NVBS
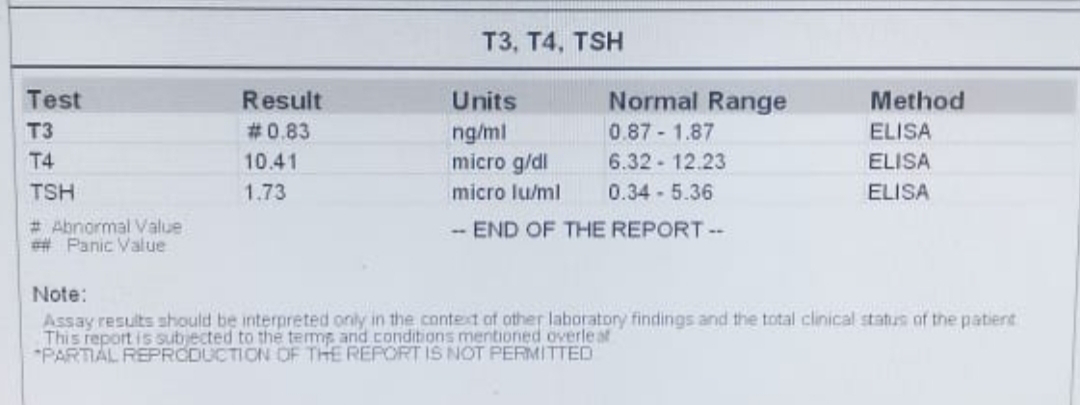
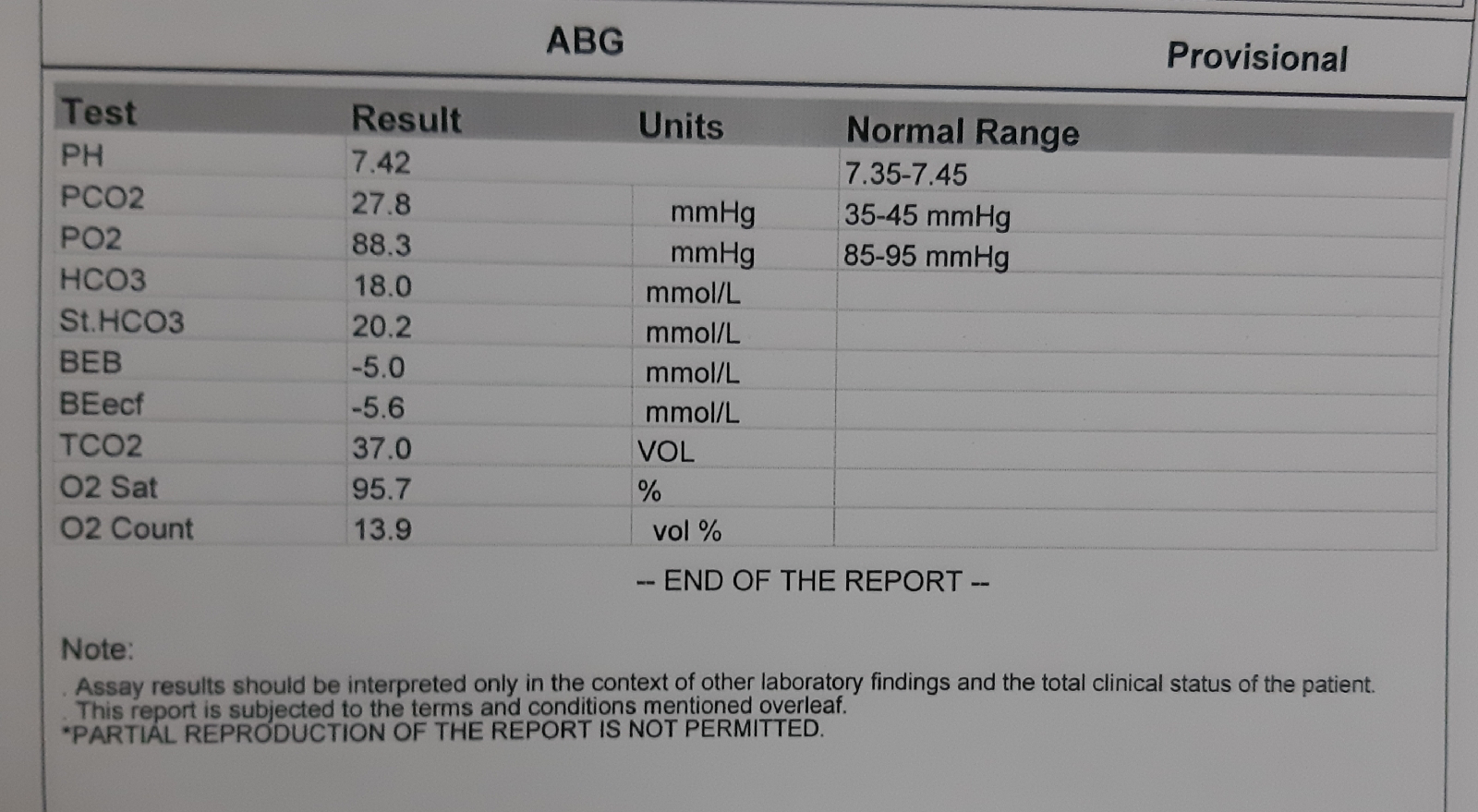
INVESTIGATIONS:
Urinary electrolytes
Na+ :216
K+ : 98
Cl- : 355
Ecg: normal




 7
7

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comments
Post a Comment