Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
CASE PRESENTATION:
A 52 year old female pt. Came to opd with 1.c/o pedal edema since 22 days
2.decreased urine output since 22 days
3.vomitings 20 days back(4-5episodes) which lasted for a day
4.sob on exertion since 20 days
5. 3 episodes of GTCS today morning
HOPI:
PT was apparently asymptomatic 22 days back then she had pedal edema ,decreased urine output , and sob on exertion for which she was admitted to a local hospital (on 23/10/2020 : .urea - 120, se.creatinine-5.3, sodium:123,k+ : 3 , hb : 9g/dl , TLC: 13660, plt: 3.44) . Renal biopsy was done on 27/10 /2020 - infection related glomerulonephritis ( IgG, C3c , C1q , kappa , lambda deposits) with 35% atrophy and vascular features of hypertension.
Pt at that time was managed with I.v antibiotics, diuretics, tolvaptan, I.v iron and supportive measures. At the time of discharge pt was started on Tab.DYTOR , TAB.OMNOCORTIN 40mgOD ,TAB.MVT ,T.TOLVAPTAN
ON 27/10/2020
Urea: 129 , creat: 4.9 , hb : 9.7
TLC : 17, 540, plt-3.71
Pt is on regular medication since then .
12/ 11/2020 : pt today presented to us with c /o SOB since morning,hiccups since yesterday,
H/O B/l pedal edema , decreased urine output , facial puffiness, abdominal distension
Nausea since yesterday night.
Pt complained of unable to speak since morning after waking up ,clenching of fists with frothing at home .After coming to hospital she had 2 episodes of tonic clonic movements of both UL and LL which lasted for 5 min and was a/w unrolling of eyeballs. Post ictal confusion lasted for 5 min. Later she was oriented well.No h/o tongue bite
No h/o fever ,cold , cough , burning micturition,pain abdomen,loose stools , NSAID abuse
K/c/o type 2 DM since 3 years and was on regular medication.
Not a k/c/o HTN ; CAD ; CVA, epilepsy
No addictions
H/O hysterectomy 8 years ago
GENERAL EXAMINATION:
PT was conscious,coherent,cooperative
Pupils :b/l NSRL
NO pallor,icterus,cyanosis,clubbing , lymphadenopathy
Pitting type of pedal edema+
VITALS:
Afebrile on presentation
Bp: 200/100mmhg
PR : 96bpm ,regular in rate and rythm
RR: 24cpm
GRBS : 214mg/dl
SPO2 : 99% AT 4L OF O2
SYSTEMIC EXAMINATION
CNS : HMF INTACT
CRANIAL NERVES INTACT
MOTOR EXAMINATION:
TONE : NORMAL IN B/L UL AND LL
POWER : UL LL
5/5 5/5
REFLEXES:
Rt lt
Biceps : 1+ 1+
Triceps : - -
Supinator: - -
Knee: 1+ 1+
Ankle : - -
Plantar : withdrawl extensor
SENSORY SYSTEM INTACT
CVS : S1 , S2 HEARD , NO MURMURS
RS: BLAE+ , NVBS
P/A : Soft, non tender
Bowel sounds +
INVESTIGATIONS:
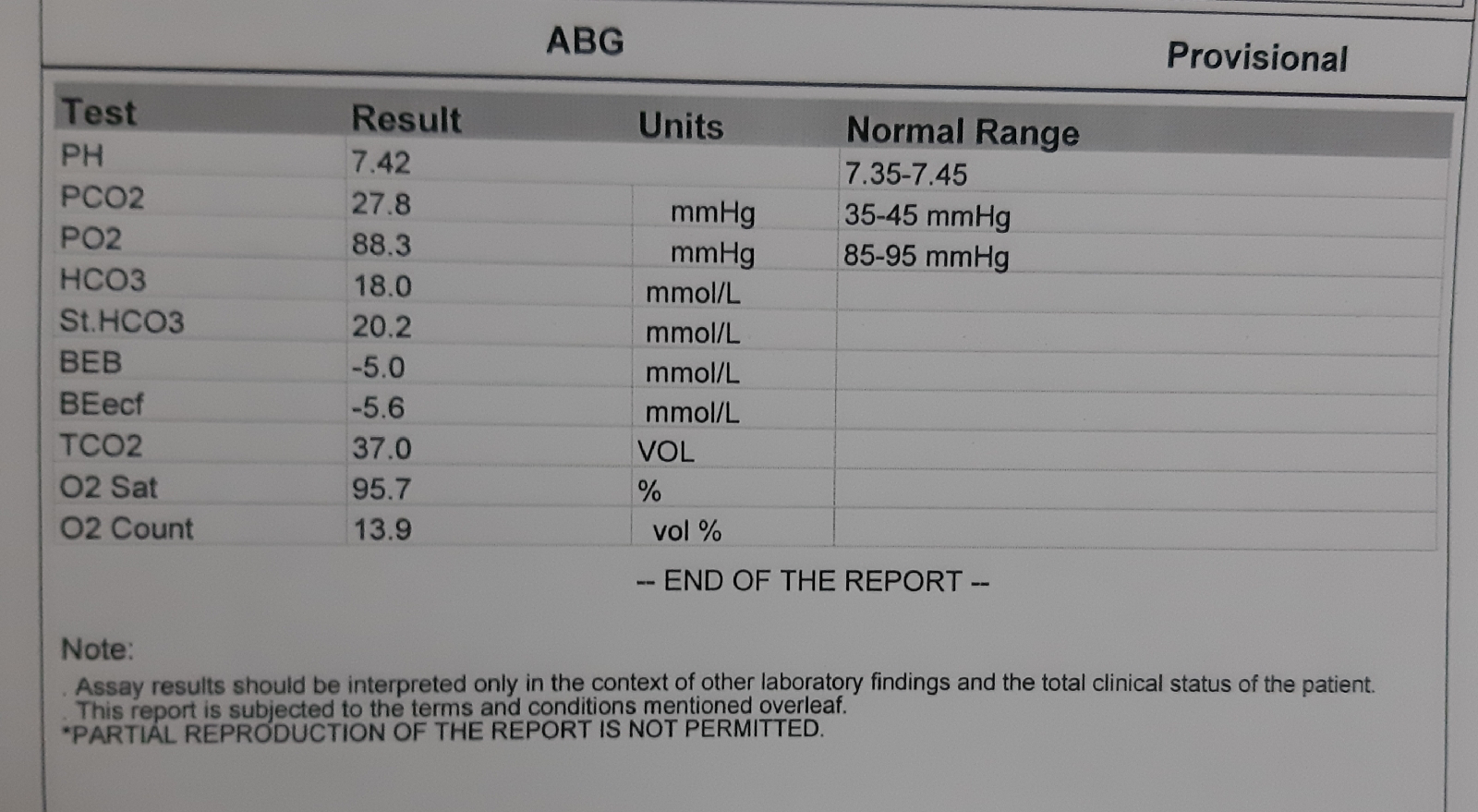
ABG
RFT






LFT

USG ABDOMEN:

Acalculous cholecystitis
B/l grade 2 RPD changes
B/l Mild pleural effusion
MRI BRAIN:

PRES, B/l chronic lacunar infarcts notes in b/l basal ganglia, corona radiata ,thalami
PROVISIONAL DIAGNOSIS:
DIABETIC NEPHROPATHY WITH PIGN
PRES( HYPERTENSIVE EMERGENCY)
ACALCULOUS CHOLECYSTITIS
2 EPISODES OF GTCS SECONDARY TO ? UREMIC ENCEPHALOPATHY?PRES
TREATMENT:



Comments
Post a Comment